I have an article online today at The New Republic where I take on both the political and economic arguments being hurled at single-payer.
Category Archives: US Health Policy
LA Review of Books: “Is the Path to Racial Health Equity Paved with ‘Reparations’? The Politics of Health, Part II”
I have a review/essay in the Los Angeles Review of Books today. It’s the second part of the “Politics of Health.” The first part mainly dealt with health inequalities by class, whereas this part deals with health inequalities by race. I review two recent books: Dayna Bowen Matthew’s Just Medicine: A Cure for Racial Inequality in American Medicine and Damon Tweedy’s Black Man in a White Coat.
#SuperTuesday
Ballot cast. Let the games begin.

560+ Physicians and Medical Students Agree: Time to Move on Medicare-for-All
More than 560 doctors and med students have signed onto an open letter organized by the Ad Hoc Committee on Medicare-for-All, now published at The Huffington Post:
The renewed debate over the merits of single-payer health reform has been marred by misleading claims that such reform is unnecessary and unaffordable. We write to set the record straight…
It’s not too late to join us: follow this link to add your signature and help turn the tide.
Time to Set the Record Straight on Single Payer
Recent weeks have seen a slew of misleading attacks on the affordability and merit of single payer health care. It’s time to set the record straight.
Please see “Setting the Record Straight on Medicare-for-All: An Open Letter From Physicians and Medical Students.” The letter went up today. You can endorse the letter on the webpage. A list of endorsers will be published in the near future. Please also circulate to colleagues. This is a crucial moment in the national debate over health care reform and single payer.
Blog: Contraception Coverage and the ACA
A “viewpoint” article published in JAMA this week (authored by March C. Politi, Adam Sonfield, and Tessa Madden) briefly summarizes how the Affordable Act Act (ACA) expands access to contraception, but also describes the various “challenges” that thus far have prevented the full implementation of this provision.
To my mind, the points they make demonstrate how the underlying, structural flaws of our health care system make even relatively straightforward and useful reforms like the ACA’s contraception mandate enormously difficult and complex to realize in practice.
As they briefly summarize in the article (“Addressing Challenges to Implementation of the Contraceptive Coverage Guarantee of the Affordable Care Act”), the ACA includes a provision that mandated that contraception-related health care – including medications, devices, services (including sterilization), office visits, and education – be covered by privates insurers without “cost sharing” (i.e. copayments or deductibles).
This is unquestionably a good and useful measure: contraception-related care is a fundamental component of comprehensive reproductive health care. There is no plausible reason to punish women who use contraception by imposing out-of-pocket payments at the time of use (the same could be said of all medically-necessary health care, in my opinion, but that’s a story for another time).
The article then briefly summarizes the various games insurers have played in preventing the implementation of this rather straightforward provision. For instance, they note that some insurers have left out coverage for certain modes of contraception (though they assert that this should be addressed by new federal rules), and also that insurers have not been reliably covering contraception-related clinical care. “Inappropriate insurance practices,” they write, “may therefore lead to patients being erroneously charged for services that should be covered with no out-of-pocket costs, potentially interfering with patients’ ability to practice contraception consistently and effectively.”
But it is when they turn to the issue of billing and coding that the ridiculous complexity of our health care system – and the harm that this complexity causes – becomes most evident. As a result of the vagaries of billing codes, what is theoretically fully covered may not be in practice. As they write:
Physicians, other clinicians, and health care organizations may find it difficult to appropriately bill for contraceptive services in a way that ensures that patients are properly exempt from cost sharing. If a patient receives contraceptive counseling as part of a well-woman examination, the situation is straightforward because the well-woman examination has a specific Current Procedural Terminology code and is considered a covered preventive service. However, if a patient has an office visit solely for contraceptive counseling (which does not have a specific billing code), the clinician or health care center must bill an appropriate evaluation and management code (which can be used for many purposes) and billing modifier (ie, 33) to specify that the visit was for the preventive service, contraceptive counseling. Many clinicians and health organizations are unaware of this modifier, and some insurers have been slow to program their billing systems so that this modifier automatically triggers the patient’s exemption from cost sharing when the included diagnosis codes (formerly International Classification of Diseases, Ninth Revision [ICD-9], now ICD-10) indicate that primarily preventive services were provided.
Of course, it is ultimately women who are penalized by this byzantine structure of coding.
But the complexities don’t end there. As they describe:
An additional challenge arises if care that involves diagnostic testing is provided during a visit, even when the initial visit was scheduled for contraceptive counseling or maintenance. Under the ACA provision, a visit should be considered preventive—and therefore exempt from cost sharing—if the primary purpose of the visit is for preventive care. However, the primary purpose may not always be clear to patients, clinicians, and payers when additional care is provided. Clinicians can use 2 separate billing codes, one for the preventive care and an additional code for the diagnostic care, but this could lead to confusion and disagreement about when patients will be charged. Greater transparency could help clinicians and health care centers communicate with patients about these potential fees.
This is of course ridiculous. In reality, office visits can be a combination of things, and attempts to classify them as purely “preventive” or not is a fiction. It’s also entirely unnecessary: if office visits for both “preventive” care and “non-preventive” both didn’t have cost sharing, none of this would matter (at least from the patient’s perspective).
They finally note that none of these protections are available for women who obtain contraception-related services “out-of-network.” Yet this may happen unwillingly: as they describe, a women may undergo a sterilization procedure at a facility that’s inside of the insurance network, but the anesthesiologist involved in the case may be out-of-network.
The story of the contraception coverage mandate of the ACA thereby speaks to the enormous difficulty of effectively – much less efficiently! – moving towards universal health care within a structure dominated by private insurers.
Blog: What Does the Medicare Rollout Say About Single Payer?

An interesting article today in Huffington Post by Steffie Woolhandler and David Himmelstein – both health policy scholars and co-founders of Physicians for a National Program – looks back at the history of Medicare for lessons about single payer today.
They make a few notable points in the piece, which is headlined “Medicare’s History Belies Claim That Medicare-for-All Would Disrupt Care.” First, they note that the implementation of Medicare was actually quite smooth. As they describe, cards were sent to the homes of all the elderly, and those who lived in more remote locations were contacted through various outreach programs; predicted doctors’ strikes never happened, and the health system wasn’t overloaded by the demands of new beneficiaries. Moreover, the process was relatively efficient: by their calculations, the rollout of the Obamacare “marketplaces” cost some seven times as much as the (inflation-adjusted) rollout of Medicare.
Second, they note that Medicare was “disruptive” in a good way: it helped undo the reign of Jim Crow medicine. As they note, the implementation of Medicare forced the segregation of Southern hospitals. At the same time, however, they rightly emphasize that de facto segregation continues today when patients with different insurance plans are treated separately. In contrast, “Medicare-for-All,” they write, “would give all Americans complete and equal coverage, completing the disruption of hospital segregation that Medicare began a half century ago.”
There is a broader point here, about the role of a true universal health care – without tiers and without financial barriers to care – in the fight against racial health inequalities. Despite all the research and discussion around the issue of “health disparities,” this issue gets insufficient attention. I discuss it in a lengthy review/essay about racial health inequality which will be published in the Los Angeles Review of Books sometime in the coming weeks.
Blog: Latest Results from the National Health Interview Survey
Uninsurance remains a problem in America, even in the age of the Affordable Care Act (ACA). That’s one conclusion that can be drawn from the latest survey results released two weeks ago by the National Center for Health Statistics.
The report (“Early Release of Estimates From the National Health Interview Survey, January–September 2015”) compares survey data on health insurance coverage gathered over the first nine months of 2015 with that of previous years, extending back to 2010. The estimates rely on a civilian, non-institutionalized sample, which for 2015 consisted of some 79,847 individuals in 37 states. I’ll briefly summarize some of the key results in this post.1
The survey demonstrates a substantial reduction in the uninsured population in the years following the implementation of the ACA. In 2010, 22.3% of non-elderly adults were uninsured at the time at which they were interviewed. In contrast, for the first 9 months of 2015, this had fallen to 12.9%. This comes after about a decade of rising uninsurance, beginning in the late 1990s:

The time trends by age groups are as one might expect. For younger adults (ages 18-24), the reduction in uninsurance occurred over 2010 and 2011. This makes sense, as the dependent coverage provision of the ACA was implemented in September 2010 (the law required coverage of children below age 26 under family health insurance plans). For other age groups, in contrast, uninsurance fell between the years 2013 and 2015. This squares with the fact that the main coverage expansion provisions of the ACA – i.e. the individual mandate and the Medicaid expansion – went into effect in 2014.
Inequalities in insurance status by class persist. In 2015, among non-elderly adults, 26.1% of the poor and 24.1% of the near-poor were uninsured at the time the interview was conducted, as compared to 7.7% of those who weren’t poor. However, there were notable reductions in uninsurance among the former two groups between 2013 and 2015:

Coverage inequalities by race – despite improvements – also persist. In 2015, among non-elderly adults, 27.9% of Hispanics and 14.6% of non-Hispanic blacks were uninsured, as compared with 8.8% of non-Hispanic whites and 7.3% of Asians:
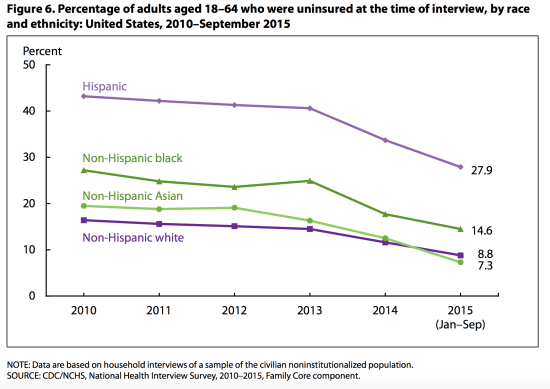
Addressing racial health inequalities, clearly, requires addressing these inequities in coverage (among many other things).
There were also inequalities by geography. Unsurprisingly, uninsurance among non-elderly adults was higher in states that have not yet expanded Medicaid under the ACA as compared to those that have (see this analysis for estimates of the number of deaths that have needlessly resulted from this “opt out”).
Finally, the survey reveals the evolving character of insurance: high-deductible heath insurance plans are on the rise. The percentage of the privately insured non-elderly with high-deductible health care plans (whether or not they are associated with a health savings account) rose from 25.3% in 2010 to 36.2% in 2015:
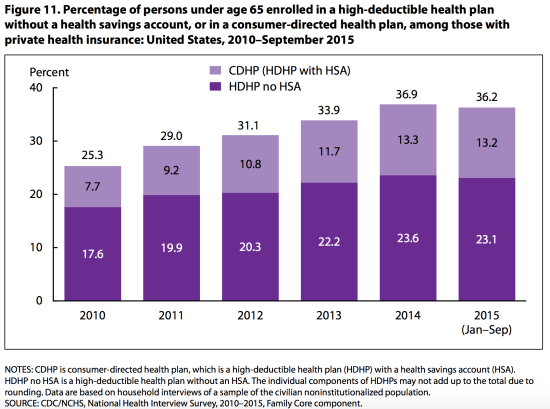
This is but one glimpse at a much larger story of rising deductibles and copayments – of underinurance more broadly – in the United States.
In sum, the ACA has clearly expanded coverage in the United States. In 2010, among those of all ages, 48.6 million were uninsured (determined based on the time they were interviewed) according to the estimates of this survey. For the first nine months of 2015, this had fallen to 28.8 million. This is no doubt a meaningfully and important change for the many millions who are now newly insured. Yet, the law is now in full effect, and millions are still excluded from coverage. Moreover, inequalities in coverage – along the lines of both race and class – persist. High-deductible health plans are on the rise. Universal health care has not yet been achieved.
————-
1 Note that all the figures reproduced here from the report are in the public domain. All numbers cited in this post are from this survey. When I say “2015,” I am referring to the first nine months of 2015. “Non-elderly adults” describes those aged 18-64.
Newsletter #2: The Single Payer Debate Continues
For now, I’ll keep posting my (brief) newsletters here. Apologies for those who come across it twice! You can signup for the newsletter here if interested: http://tinyletter.com/awgaffney
———————
Dear PP Subscribers,
The Democratic primary race has intensified. Contests in Nevada and South Carolina are looming. The debate over single payer remains fierce.
The last few weeks have seen continued arguments from a spectrum of commentators as to why a Medicare-for-all program – like that proposed by the Sanders campaign – is untenable.
A number of overlapping lines of argument can be distinguished. First, it is frequently argued that the Sanders plan is poorly formulated and/or unrealistic given political conditions in Washington. Recently, for instance, Paul Starr in the American Prospect (headlined “The False Lure of the Sanders Single-Payer Plan”) argues that the Sanders proposal is “not a practical or carefully thought-out proposal.” Indeed, he sees the plan as an indictment of his overall campaign: it’s “a symbolic gesture, representative of the kind of socialism he supports.”
I addressed some of the earlier (and similar) liberal criticisms in an article published January 21 in US News & World Report, “Single Payer is Worth Fighting For.” I conclude:
The expansion of coverage achieved by the Affordable Care Act does not constitute a system of universal health care. Too many are uninsured and underinsured. Too many are squeezed by high deductibles, contend with “narrow networks” of doctors and hospitals, or face crushing medical bills and even bankruptcy. Single-payer is the best way to remedy these injustices while simultaneously controlling overall health spending.
I also chatted about some of these issues on the radio with Arnie Arnesan on WNHN 94.7, available here.
A second line is that single payer is simply not affordable – that the number don’t add up. For instance, in casting doubt on the seriousness of the Sanders’ single payer proposal, Starr relies on the widely-covered estimates of Kenneth Thorpe, an economist at Emory University. Vox covered Thorpe’s new estimates, which put the price of Sanders’ single payer proposal at nearly twice what his campaign has contended.
However, David Himmelstein and Steffie Woolhandler have clearly demonstrated the flawed assumptions behind these numbers in this detailed post at the Huffington Post, which is well worth reading. As they put it:
Thorpe’s analysis rests on several incorrect, and occasionally outlandish, assumptions. Moreover, it is at odds with analyses of the costs of single-payer programs that he produced in the past, which projected large savings from such reform […] In the past, Thorpe estimated that single-payer reform would lower health spending while covering all of the uninsured and upgrading coverage for the tens of millions who are currently underinsured. The facts on which those conclusions were based have not changed.
A third line admits the shortcomings of the current state of affairs in American health care, but suggests that the right way forward would be to expand towards universal coverage under the ACA – instead of pursuing the more fundamental change of single payer. I address this argument in an article published online Thursday in Jacobin, headlined “What Obamacare Can’t Do.” I turn to a country that has attempted to work towards “universal” coverage through a system of competing private insurers – the Netherlands – to demonstrate why this approach falls short, both from the perspective of cost and efficiency as well as that of equity.Regardless of the outcome of the primary, the campaign for single payer debate is far from over. The incremental reforms have already been accomplished – we now either move backwards or we move ahead.
Until the next sporadically timed newsletter,
Adam
Post lightly edited.
Blog: Implications of a Tight Race
The Democratic primary race has grown tighter and spicier than virtually anyone had predicted. A quick glance at February:
Looking back:
February 1: Hillary Clinton bests Bernie Sanders in the Iowa caucus, but only by the narrowest of victories.
February 5: A national poll puts Clinton and Sanders in a dead heat: as Politico reported, Sanders is at 42% compared with Clinton at 44%. These percentages fall within the margin of error.
February 9: Sanders dominates the New Hampshire primary by a margin of more than 20 points. But perhaps just as important, as David R. Jones noted in a post in The New York Times, Sanders won in essentially all categories of voters:
He carried majorities of both men and women. He won among those with and without college degrees. He won among gun owners and non-gun owners. He beat Mrs. Clinton among previous primary voters and those participating for the first time. And he ran ahead among both moderates and liberals.
February 12: As the Hill reports, another poll demonstrates a tight race, with Clinton having only a 7-point lead over Sanders nationwide.
Looking forward:
February 20: The next Democratic contest, the Nevada caucus. Recent reliable polls seem to be in short supply. For what it’s worth, FiveThirtyEight’s “polls-plus” analysis gives the two candidates an equal chance of winning. On Friday, Slate’s Jim Newell described Clinton’s numerous advantages in the state – her so-called “Western firewall” – but also notes that “it wouldn’t be surprising if this firewall is crumbling, or whatever it is that firewalls do when they stop being firewalls.” Do they smolder, or are they quenched?
February 27: The South Carolina primary. This is seen as Clinton’s real “firewall,” as the odd saying goes. According to FiveThirtyEight, she is set to dominate the state. However, a long report, well worth reading, by Joyn-Ann Reid at MSNBC headlined “Warning signs for Hillary Clinton in South Carolina” argues that the situation in that state may be less settled than polls may suggest.
Time will tell. In the meanwhile, the tightening of the race has meant that single payer health care has remained front and center of the national political discussion. For single payer advocates it is a crucial time to continue pressing the cause.
Jacobin: “What Obamacare Can’t Do”
Today in Jacobin, I write about why single payer remains critical to the goal of universal health in the US – and why other roads will fail.
Chatting Single Payer with Arnie Arnesen
Arnie Arnesen kindly had me back on her radio program “The Attitude” on WNHN 94.7 FM in Concord, NH to chat about the politics and policy and history of single payer. Podcast is available here.
US News & World Report: Single-Payer Is Worth Fighting For
I have an op-ed today on why the naysayers are wrong about single-payer, available here.
Blog Post: Comments to the Washington Examiner
The Washington Examiners‘ Robert King had an article today about the ongoing single payer battle, “Sanders reignites fight over single-payer healthcare“.
The article notes that though some would contend that the debate over incrementalism vs. more fundamental reform is already behind us, “…single-payer advocates beg to differ.” In this case, I was the single-payer advocate doing the begging:
“The Affordable Care Act didn’t address a lot of the problems in the [healthcare] system,” said Adam Gaffney, a physician, writer and single-payer advocate. Gaffney said his views don’t represent any groups he is affiliated with.
Cost-sharing requirements such as co-pays and deductibles have increased, and more than 30 million Americans are underinsured, Gaffney said.
“Regardless of what happens in the coming general election, the Affordable Care Act will not have killed single payer,” he said.
Gaffney said he was disappointed that Clinton seems to be “closing the door on a single-payer program given that so many people support it.”
Available at: http://www.washingtonexaminer.com/sanders-reignites-fight-over-single-payer-healthcare/article/2580856
Blog Post: What’s wrong with Matt Yglesias’ Single Payer Analysis
Does single payer save money? Matt Yglesias had a piece in Vox today headlined “The single-payer debate we should be having,” in which he admits that Hillary Clinton’s recent anti-single payer (SP) attack is “questionable,” but contends that we’re missing the main point about SP: namely, that it saves money by reducing reimbursement to health care providers like physicians.
Such a move would be politically very difficult, he argues, and in any event we could very well cut payments without moving to SP – and save money all the same. It’s best to quote him at length:
Single-payer systems save money by squeezing health care providers — doctors, hospitals, and ultimately everyone who works for them — which would be very difficult to accomplish ex post facto. If the political consensus did exist for enacting large, across-the-board cuts in doctors’ fees and hospital charges, then there would be no need to shift to a single-payer system in order to accomplish the cuts. In the absence of such a consensus, the switch to single-payer actually wouldn’t save money, and the costs would become exorbitant.
Thus, he contends that “a single-payer structure is neither necessary nor sufficient” to reduce health expenditures in this fashion. He says a lot in this article, some of which is fair, but this specific point is incorrect.
In passing, Yglesias briefly mentions that SP would be administratively simpler, yielding some increased efficiencies. But this is entirely inadequate: reduced administrative expenditures would be a primary source of potential savings under SP. This may sound wonkish, but it’s a point of great importance in this very high-stakes debate.
There’s a whole literature about administrative inefficiencies of the US health care system, but I’d ask Yglesias to have a look at this paper by Jiwani et al., Billing and insurance-related administrative costs in United States’ health care: synthesis of micro-costing evidence, published in BMC Health Services Research in 2014 (note: two of the co-authors [DS and SW] are colleagues/collaborators on other projects). The paper provides an estimate for “billing and insurance-related” (BIR) costs for the US health care system, and compares it to Canada, which has a single-payer system.
The potential estimated efficiency savings are enormous. In comparison to the SP system in Canada, “added BIR costs” were estimated at $49 billion/year for physician practices, $54 billion/year for hospitals, and $69 billion/year for “other health service and supplies.” Using US Medicare as a benchmark, added BIR costs were estimated at $185 billion/year for private insurers and $18 billion/year for public insurers. Depending on the exact assumptions used, the investigators produced a “plausible range for overall added BIR costs in the US of $254 – $507 billion in 2012…”
The implications of this are clear: the efficiencies of a SP system – which could reduce or eliminate the need for a whole range of administrative and billing activities at the level of insurance companies, hospitals, and doctors’ offices – could be a substantial contribution towards expanding coverage under SP. To quote the investigators:
Implementation of a simplified financing system offers the potential for substantial administrative savings, on the order of $375 billion annually, which could cover all of the uninsured and upgrade coverage for the tens of millions who are under-insured.
This might sound farfetched for those who are unfamiliar with the enormous administrative inefficiency of the US health care system. Hospitals, for example, currently tabulate complex patient-by-patient bills, sometimes for every service or supply utilized (and often chase down those with unpaid bills using debt collection agencies). Under SP, they could instead be paid “global budgets” to cover all operating expenses and all patients; the need for hospital billing departments would thereby shrivel. Physicians practices’ likewise must bill (and jostle with) an ever-changing roster of insurance plans, requiring significant staff and/or time.
In short, Yglesias’ analysis of the current SP debate almost entirely neglects how increased administrative simplicity could pay for a SP system that eliminated both uninsurance and underinsurance. Even if overall health care expenditures were unchanged at the end of the day, this would be quite a bargain.
Blog Post: Chelsea Clinton Grossly Misrepresents Single Payer
Chelsea Clinton isn’t just a political surrogate, she’s someone who purports to know something about public health. She is, after all, the Vice Chair of the Clinton Foundation, where – according to its website – she works on the organization’s multiple public health projects. More to the point, she is an adjunct assistant professor in health policy and management at the Columbia Mailman School of Public Health, where she earned her Masters in Public Health degree.
Which makes her gross misrepresentation of Sanders’ health plan only that much more contemptible. “Sen. Sanders wants to dismantle Obamacare, dismantle the CHIP [Children’s Health Insurance] program, dismantle Medicare, and dismantle private insurance,” she was quoted as saying by MSNBC while on the campaign trail for her mother in New Hampshire. She continued (again as quoted by MSNBC): “I worry if we give Republicans Democratic permission to do that, we’ll go back to an era – before we had the Affordable Care Act – that would strip millions and millions and millions of people off their health insurance.”
This would be an absurd interpretation of Sanders’ single payer proposal for anybody, much less for someone with some background in health policy. It doesn’t seem to have been an off-the-cuff remark, however: it mirrors a somewhat similar comment made by Hillary Clinton the day before. As she was quoted by the Washington Post:
His plan would take Medicare and Medicaid and the Children’s Health Insurance Program and the Affordable Care Act health-care insurance and private employer health insurance and he would take that all together and send health insurance to the states, turning over your and my health insurance to governors.
Now I’m a single payer advocate, active in the organization Physicians for a National Health Program (though the views expressed in my articles and blog posts are mine only). If you don’t agree with the vision of a single payer program – whether because you think private insurers do a right proper job of delivering a right to health care or because your campaign receives generous funding from the pharmaceutical industry or whatever – so be it.
But don’t grossly misrepresent such a system by suggesting that Sanders would “dismantle Medicare,” as Chelsea Clinton did. Particularly not when the text of Sanders’ 2013 single payer bill states, “…the 113th Congress should enact a Medicare-for-All Single Payer Health Care System…” This bill is one of several single payer bills and proposals. Representative John Conyers’ single payer bill, H.R. 676, is in fact named the “Expanded & Improved Medicare For All Act.” To suggest that a system that would provide an improved Medicare program universally to the nation would somehow sneakily rob seniors of their Medicare coverage demonstrates a rather poor grasp of the issues (or something worse).
What both Clintons’ seem to be alluding to, as The Week’s typically on-point Ryan Cooper described earlier this week, is the fact that Sanders’ 2013 bill configures a single payer plan that would, to some extent, have a state-based administrative structure (though it would still be a federal plan and be implemented in every state). Cooper contends that there are some reasonable objections to such a structure, and that perhaps an entirely federal plan might well be superior.
Yet these are relatively minor details. To characterize Sanders’ single payer platform as some sort of dispersal of health care to the whim and fancy of each individual state is fantastically inaccurate. Sanders’ has proposed a fundamentally universal system: a national health program that would cover essentially everyone in every state. At that point, we wouldn’t need a separate Medicaid or Medicare program (or private insurer), which is the raison d’etre of “single payer.” Such a system would be far more just and equitable than what we have now, where – even with the Affordable Care Act largely intact – 32 million remain uninsured and another 31 million underinsured, among other failings.
Of course, such issues will never be a problem for Chelsea Clinton, primarily because she is part of a fabulously rich family. Indeed, as the Intercept’s Zaid Jilani described yesterday in a good piece entitled “Hillary Clinton’s Single-Payer Pivot Greased By Millions in Industry Speech Fees,” Hillary Clinton has raked in a cool $2.8 million in speaking fees in the past two years from the health care industry alone. Jilani also notes that Bill Clinton gave a speech (one presumes for a hefty fee) last year for America’s Health Insurance Plans, the main lobbying group for the health insurance industry. And Chelsea Clinton herself is already able to command $65,000 per college speaking gig, according to the Washington Post.
Like her parents, in other words, Chelsea Clinton is unlikely to go broke from a sky-high deductible or because she inadvertently went to an “out-of-network” doctor or hospital; she’ll never be forced to choose between filling a prescription and paying for rent. Nor should she – nor should anybody.
But obviously that’s no excuse for a campaign surrogate (much less an adjunct assistant professor of health policy and management) to so grossly mischaracterize a rather familiar health reform proposal, particularly not one that has the potential of improving – indeed saving – the lives of so many.
Jacobin: Your Life or Your Wallet
Today in Jacobin I take on the case of skyrocketing pharmaceutical prices – exemplified by the price hike of pyrimethamine – and discuss how we might create a more just pharmaceutical framework.
Wall Street Journal’s $15 trillion Single-Payer “Price Tag”
An article published in the Wall Street Journal today, headlined the “Price Tag of Bernie Sanders Proposals: $18 Trillion,” seems intended to induce what I might call “single payer sticker shock.” After all, the article states, $18 trillion not only “alarms conservatives,” but also “gives even many Democrats pause.” $15 of that $18 trillion is attributed to Sanders’ proposed single-payer health care reform. It sounds like a forbiddingly high number.
But is it a fair number? A story by David Dayen at The Intercept (“Wall Street Journal’s Scary Sanders Price Tag Ignores Health Savings) and a post by Matt Yglesias at Vox (“Bernie Sanders’ $18 trillion in proposed spending is more affordable than it sounds”) help put this number in context, but I think there are couple more things to be said about it.
As Dayen notes, the article draws from a study published by Gerald Friedman, an economist at the University of Massachusetts at Amherst, to compute the $15 trillion figure. Friedman wrote the study in 2013 in order to estimate how HR 676 – the single-payer bill sponsored by Congressman John Conyers – might be financed. The mix of taxes Friedman suggests is one potential approach to paying for single-payer; others are possible.
In any event, since the WSJ article relies on Friedman’s estimate, it’s worth turning to his report and asking: how much would single-payer cost? There are two ways to answer this question.
In Table 2, Friedman describes the “Estimated costs of health system improvement and transition costs under HR 676 (in billions of dollars),” which I’ve reproduced, verbatim, here:
| Increased utilization | $144 |
| Cost of expanded coverage including government administrative costs | $110 |
| Cost of Medicaid rate adjustment | $89 |
| Transition cost of unemployment insurance and retraining for displaced workers | $31 |
| Transition cost of capital buy-out of private health care facilities | $20 |
| Total | $394 |
Thus, according to Friedman’s analysis, the cost of expanding health coverage to everyone in America (i.e. eliminating uninsurance together with most out-of-pocket health care costs) along with various associated costs (e.g. reimbursing owners of for-profit health facilities and assisting newly unemployed insurance workers) would cost $394 billion annually ($51 billion of that would be for transitional costs, so would apply to the first year only).
So should we argue that single-payer “costs” $394 billion a year? No, we shouldn’t. Table 3, “Savings on provider administrative overhead and pharmaceutical costs,” details the various savings associated with a single-payer system. Direct governmental negotiation with pharmaceutical companies over drug prices would result in $115.9 billion savings annually. Reduced administrative expenditures (something I recently blogged about), would, according to Friedman’s numbers, save $476 billion a year.
In other words, at least according to this one study, overall savings under HR 676 would be $592 billion a year, while overall costs would be $394 billion a year. Here is Friedman’s pie chart, which I’ve redrawn:

Now, as Dayen argues, this makes sense: “The entire point of a single-payer health care plan, aside from covering everyone in the country,” he writes, “is to minimize costs, by reducing administrative bureaucracy, the profit motive and middlemen.” Exactly. But if savings > costs, where does the $15 trillion figure come from?
In a universal single-payer health care system, everyone would be covered; all current expenditures on health care would be replaced by taxes. As the WSJ admits, the “trade-off” for such new taxes would be that “employers would no longer have to pay for or arrange their workers’ insurance.” However, this is entirely inadequate. The following additional expenditures would likewise disappear entirely:
1) Employee contributions to their insurance premiums
2) Payments made for insurance premiums for those not covered by their employer.
3) Out-of-pocket expenditures (which are on the rise) on things like copayments, deductibles, and co-insurance
4) Payments for long-term care, which are today essentially uncovered for most (except for those in poverty, through Medicaid)
Yes, all of those payments would have to be replaced by taxes (see note 2 below). But as Yglesias notes, “[i]f you financed it [single payer] with a broad-based payroll tax (the way Social Security is financed), people with job-based insurance plans wouldn’t even notice the difference — today’s insurance premium line on your pay stub would become a tax line.”
While payroll taxes are only one way to finance single-payer (and, as the 2003 PNHP proposal notes, progressive taxation would actually be fairer), the overall principle holds: replacing current health care expenditures with taxes would be relatively unobtrusive for most of us.
And in return for what is essentially a spending swap, we would have universal first-dollar health care for everyone in the nation. That seems, to me, to be a small price to pay.
Note: Edited for unfortunate name misspellings … Apologies! Also, my initial figures for administrative (and total savings) were incorrect in the text, though they were correct in the pie chart; they have now been corrected. Finally, I’ve now clarified that of Friedman’s $394 billion per year in costs for health system improvement under single-payer, $51 billion would be for transitional costs which would apply for the first year only.
Note 2: How much would those payments be? Although the $15 trillion figure is sourced in the WSJ article to Friedman’s study, the study that I linked to doesn’t mention that number. I’m assuming the figure combines the assumptions of the study with projected national health expenditures over the next ten years (figures noted by both Dayen and Yglesias), which are available from CMS here (NHE Projections 2014-2024, Table 3 “National Health Expenditures By Source of Funds”). Summing the projected national health expenditures for the years 2014 – 2023 gives us $4.14 trillion in projected out-of-pocket payments and $13.16 trillion for private health insurance. Those sources of payment would need to be replaced with public funding. Doug Henwood also pointed to this data, and made a similar overall point, at LBO.
Note 3: I’ve noticed that Gerald Friedman, the author of the study cited by the WSJ, has weighed in on the use of his analysis at the Huffington Post, available here. He includes his 10-year projections, and confirms that approximately $15 trillion in new federal spending would be required under HR 676. However, “…by spending these vast sums,” he writes, “we would, as a country, save nearly $5 trillion over ten years in reduced administrative waste, lower pharmaceutical and device prices, and by lowering the rate of medical inflation.” The bottom line couldn’t be clearer.
CNN: Racial injustice still rife in health care
Racism mars the history of health care in America. For years, black patients were relegated to separate — and appallingly unequal — hospitals and wards. Many were simply denied medical attention, either “dumped” into the care of other facilities or turned away at the hospital door … An Op-Ed by me and Vijay Das of Public Citizen at CNN.com today.
Blog Post: Hayek and Healthcare Administrative Expenditures (not at all wonkish)
Would a single-payer national health program, at the end of the day, truly be sleeker and slimmer than our bloated and fragmented semi-private system? Not according to Dr. Michel Accad, who takes on this important single-payer talking point in his blog post posted last week on KevinMD, “Will single-payer really reduce administrative waste?”
Given that savings from reduced expenditures on billing and overhead are a core argument that single-payer advocates (myself among them) employ to advance our cause, the piece caught my eye. To quote the proposal of the Physicians’ Working Group for Single-Payer Insurance (of note, I’m active in the organization Physicians for a National Health Program, which was behind the proposal), published in JAMA in 2003:
Our multiplicity of insurers forces US hospitals to spend more than twice as much as Canadian hospitals on billing and administration; forces US physicians to spend vast amounts on billing; and nourishes a panoply of business consultants, coding software vendors, and other satellite business.
So had a new study been published demonstrating, contrary to all existing data, that private insurers somehow had lower administrative costs than Medicare? Had Canadian expenditures on healthcare administration somehow suddenly vaulted ahead of that of the United States?
No, neither had come to pass (not surprisingly). In fact, Dr. Accad doesn’t really deal with any of the literature about the administrative efficiency of different types of health care systems. Instead, he employs a “Hayekian perspective” to make the argument that central economic planning is inherently inferior to an atomized free market where individual economic actors buy and sell, rationally relying on their intimate knowledge of local market circumstances. “Only in a decentralized system,” he argues, “of decision making, where price fluctuations can adjust to the reality of needs and provisions, are major gluts and shortages avoided.” (i.e. no one knows the business of bread making better than the bread maker, etc. etc.).
Now on the one hand, it’s a bit quixotic to invoke the political philosophy of a neoliberal economist to argue against what is essentially empirical point, i.e. that the United States spends more on health care administration than nations that have a single-payer system.
For it clearly does. To review, one 2003 study published in the New England Journal of Medicine found that the US spent about three-times as much as Canada on health administration ($1,059 vs. $307 per capita, in 1999). More recently, a study published in Health Affairs found that the US had the highest hospital administrative costs among eight high-income nations (an astronomical 1.43% of GDP spent annually on hospital administration in the US, as compared to 0.41% in Canada).
Closer to home, Medicare – a single-payer-like system for older Americans – has an administrative overhead around 2%, as compared to the 13.6% in overhead and profits of privatized Medicare Advantage, which is run by private insurers.
I could quote my favored political philosophers here to counter Accad’s quotes from Hayek, but it’s really all beside the point. “The question,” as the Princeton health care economist Uwe E. Reinhardt put it in a post on the issue in New York Times, “is how long American health policy makers, and particularly the leaders of our private health insurance, can justify this enormous and costly administrative burden to the American people and to the harried providers of health care.”
To be fair, Dr. Accad makes a good point ridiculing the extraordinarily complex and “byzantine scheme of codification” used by Medicare (and followed by private insurers) for billing purposes. “[A] CPT code 99204-21 (new patient visit, E/M coding level 4, prolonged service) associated with ICD-9 code 786.50 (chest pain, unspecified),” he notes, “hardly conveys any real knowledge and cannot possibly be a basis on which relevant decisions can be made or value established.”
No, it can’t, but that’s not what such codes are used for: they’re used to determine reimbursement. But they don’t have to be – and that’s where the administrative savings come in.
Under a single payer system (as PNHP’s proposals describe), hospitals would receive a global lump sum budget to pay for all operating costs; there would be no need to monitor services used by individual patients, tabulate costs, or hire debt collectors. Indeed, hospital billing could largely be eliminated from the ledgers of hospital operating expenses.
Simplified fee schedules, capitation, or salaries – without bonuses or penalties for more or less health care use – would be used to reimburse providers in the outpatient sector. The name of the game would be “[s]implicity, simplicity, simplicity!”, as one prominent New Englander put it in his important defense of a national single-payer system, Walden.
I share what I sense is Dr. Accad’s bitterness at onerous documentation obligations. But a universal system would make much of that documentation irrelevant, and therefore unnecessary. It would therefore be a win both for practitioners and for the public (though it would admittedly be a loss for many others, including those who profit from the system’s inefficiency, e.g. the health insurance industry).
“Reducing administrative waste” may or no not be the heady revolutionary slogan that today’s millennial physician-activists are looking for, but it’s no less true for that – whatever the unrelated musings of Hayek or Henry David Thoreau.
Note: Updated to note that the “global lump sum budget” is described in PNHP’s proposals.
Note 2: A version of this post has been published on KevinMD.com.
